
Super Staph in the Community: Is It Evolving?
Abstract
Staphylococcus aureus infections are a common cause of disease, particularly in colonized people. They frequently cause staph infections and are often dubbed “Super Staph” because they are virulent and multidrug resistant. Recently, a series of published articles have reported that community-acquired methicillin-resistant S. aureus (CA-MRSA) strains are evolving and becoming more prevalent in households. In contrast, health care acquired MRSA (HA-MRSA) is declining in the United States. The changing “Superbugs” have often been used as an example of “evolution in action.” Although MRSA infections have become more prevalent in the community, studies of college students carrying S. aureus and MRSA colonization are lacking. In early studies at Liberty University, we have found that students in microbiology classes who have more contact with individuals in a healthcare setting are more likely to carry MRSA in their body. The classes that had the highest rate of HA-MRSA carriage were those primarily populated by nursing students. Nursing students typically have greater exposure to clinical settings and nursing homes than students in other fields of study. However, in research collected this past year, 2014–2015, we observed a shift to students of many majors now carrying CA-MRSA.
At Liberty University, we sampled 544 students and had up to 20%+ MRSA rates common among clinically oriented students, five to ten times the national average. We have seen a changing profile from HA-MRSA to CA-MRSA; this change has the potential to be dangerous, since the new strains are more virulent and aggressive. CA-MRSA is somewhat difficult to define, but is mostly associated with antibiotic profile, toxin genes, and place of acquisition. There is a variation of S. aureus strains, but most change is found in tightly knit groups: households, dorms, and other close living quarters. The bacteria are “ping-ponging” around among students, changing as they go.
This change is real and clearly indicates an emergence of new MRSA variants that some may call microevolution. It is, however, not Darwinian upward-onward evolution but clearly adaptive changes within a species: variants on a theme. MRSA strains are acquiring more genes as they “ping-pong” from one person to another. They change their virulence as they pick up more foreign genes (via phage or plasmids) and vary as they go.
The purpose of this article is to provide a reasonable explanation for the genesis, emergence, and the new dominance of Community-associated (CA) MRSA. It also addresses the issue of whether this phenomenon is “evolution in action.” Microbiology research based on the creation paradigm appears to provide some answers to these puzzling questions regarding the new variants of Staphylococcus aureus and its emerging dominance in the United States.
Keywords: Staphylococcus aureus, MRSA, Super Staph, CA-MRSA, HA-MRSA, Evolution of MRSA, Superbugs
Introduction
MRSA bacteria frequently cause staph infections and are often dubbed “Super Staph” because they are virulent and multidrug resistant. MRSA is rapidly becoming one of the most prevalent and menacing diseases of our time and makes time spent in a hospital an increasing risk. MRSA are bacteria that represent “new” strains of antibiotic-resistant Staphylococcus aureus (figs. 1–2). Although the media discusses MRSA as a single new strain, in reality MRSA represents more than 1100 distinct strains of S. aureus (Gillen 2009). S. aureus causes many diseases (fig. 3), including skin boils and infection of leg ulcers, pressure sores, or any open wounds. Occasionally, it can cause more serious disorders such as pneumonia, or infection of the blood (septicemia), bone, joint, or heart valve. The virulence factors and their resistance to antibiotics make MRSA bacteria deadly. In the late 1990s a resistant strain was found to be a community-acquired methicillin-resistant S. aureus strain. Unfortunately resistance has increased dramatically since 2000. Several national studies report that more people carry MRSA in communities than hospitals.
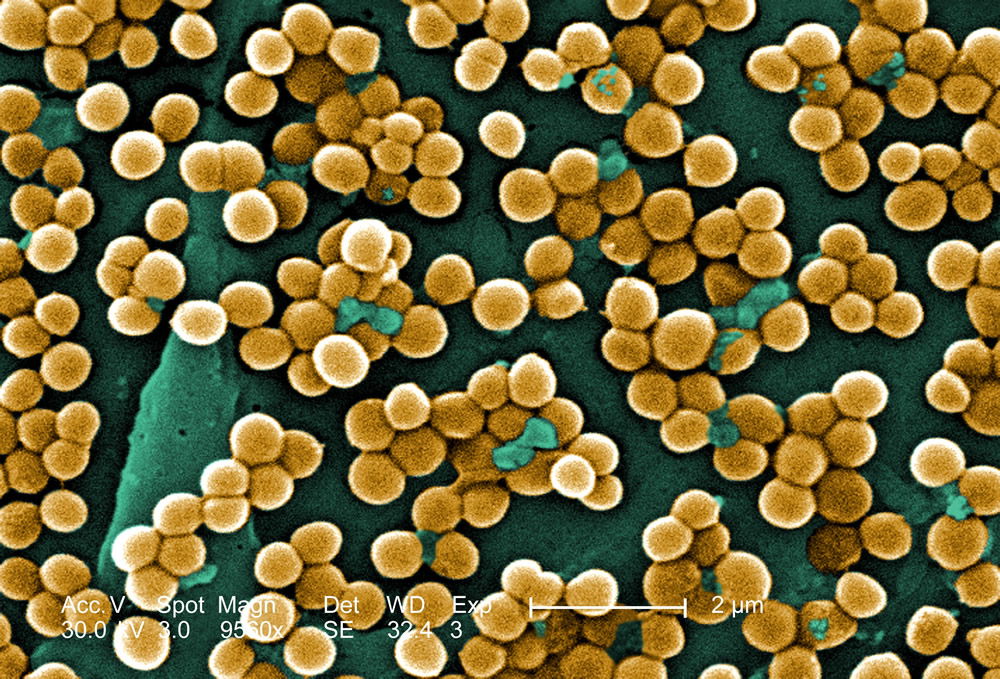
Figure 1. Scanning electron micrograph (SEM) depicting numerous clumps of methicillin-resistant Staphylococcus aureus (MRSA) in gold, magnified 9560x. (Wiki Commons and CDC stock photo) see Gillen, 2009 article
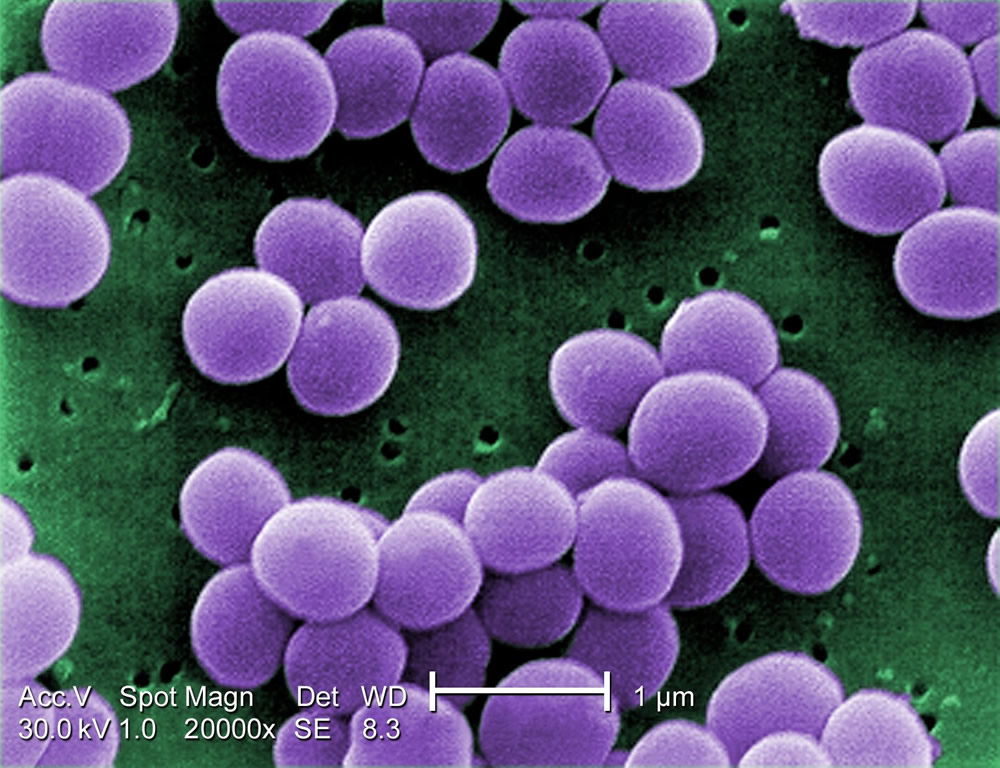
Figure 2. Scanning electron micrograph (SEM) depicting Staphylococcus aureus, in purple, magnified 20,000x. (Wiki Commons and CDC stock photo).

Figure 3. Cutaneous abscess, MRSA. Courtesy of Wikimedia.
These bacteria are now categorized as Hospital-associated MRSA (HA-MRSA) and Community-associated MRSA (CA-MRSA) depending upon the disease acquisition location.
HA-MRSA and CA-MRSA are similar in many ways, but distinct. HA-MRSA has an antibiotic resistance to many antibiotics and is sensitive to Cipro (a fluoroquinolone antibiotic) whereas CA-MRSA has an antibiotic resistance to few antibiotics and is Cipro-resistant. Genetic traits for CA-MRSA include a gene that destroys leukocytes and a special chromosomal gene of USA300 types. CA-MRSA tests positive for leukocidin (PVL) and other toxins. HA-MRSA does not usually contain these toxins (Table 1). It is this PVL toxin that makes the USA300 strain very dangerous. CA-MRSA commonly enters the blood stream through the lungs, surgical sites, and implant sites. However, it may also affect a portion of the skin appearing as a “spider bite,” pimple, or boil that is inflamed and swollen.
| MRSA in Health Care | MRSA in the Community | |
|---|---|---|
| Major Genotypes | USA100/200 | USA300/400 |
| Antibiotic Resistance |
Many Antibiotics/Antimicrobial medications Cipro-sensitive |
Few Antibiotics/Antimicrobial medications Cipro-resistant |
| Virulence Factor | HA-MRSA | CA-MRSA |
| SCCmec1 | Types I – III | Types IV, V |
| Leukocidin (PVL) | ─ | + |
Community-associated MRSA (CA-MRSA) was initially defined as infection of MRSA in an outpatient, or a patient released from the hospital or clinic within 24 hours (Fox et al., 2015). However, it is now recognized that CA-MRSA has unique characteristics not related to hospitalization or time released from a health care facility. CA-MRSA has a unique genetic profile, antibiotic sensitivity/resistant pattern, epidemiology, presentation, and treatment. Ciprofloxacin (Cipro) resistance is due to the mutation of one gene base, and we choose this trait as a “marker” because it is easy to identify using the standard lab test. A recent study (ASM, 2015) reveals that a large proportion of the USA300 isolates sequenced are resistant to ciprofloxacin antibiotics. The significance of their study is that if households serve as long-term reservoirs of USA300, household MRSA eradication programs may result in a uniquely effective control method.
Liberty University Research Verifies National Research
The methods we used to do research are given more completely in a previous study (Gillen, Daycock, and Serafin, 2014). At Liberty University, we sampled 544 students and had 20%+ MRSA rates common among clinically-oriented students, five to ten times the national average. In particular, we compared students carrying MRSA in 2013–2014 versus 2014–2015 and found more CA-MRSA this past year. We asked: Has the distribution of MRSA carriage origin changed from year to year among nursing students? Yes. In 2013–2014, we only found 3% had CA-MRSA; whereas, in BIOL 2014–2015 we found 8% had CA-MRSA.
In another Liberty University study, 332 dorm students were sampled and it was found that students living in close-knit dorms (community shared bathrooms, etc.) had a much higher (8.4%) than those in spaced dorms (1.5%) CA-MRSA rate. Those in spaced dorms had a rate similar to the national average (2%). We have also seen a changing profile from HA-MRSA to CA-MRSA; this is potentially dangerous since many of these new strains are more virulent and aggressive.
There was an overall trend change of MRSA among the Liberty University student population. A shift from HA-MRSA to CA-MRSA among the Liberty University student body over the 2013–2014 and 2014–2015 school years is evident after testing. There has been a rise in CA-MRSA from 2013 to 2015. The surveys indicated the prevalence of HA-MRSA among nursing majors with clinical experience, while other carriers who lacked clinical experience typically harbored CA-MRSA. Distinguishing HA-MRSA from CA-MRSA was accomplished by discovering the strain’s lab tests. A more detailed research report is available in .
Our conclusion coincides with a study done by the University of Chicago that analyzed a growing trend of CA-MRSA (USA300) carriage in major cities across the United States of America (Alam et al., 2015). The rapid change within CA-MRSA could be explained by the “Ping-Pong Phenomenon” (fig. 4). If the ball hits a paddle that has a “sticky” gene, then hits another with a second gene, and finally, a third gene, the end result would be all genes attached to the ball. In similar fashion, if a S. aureus coccus carrying unique bacterial DNA enters one person, and then two more unique variants invade a second and third person in the same family, the individuals of this family may carry any combination of the three new DNA strips, and thus, different MRSA isolates (fig. 4).
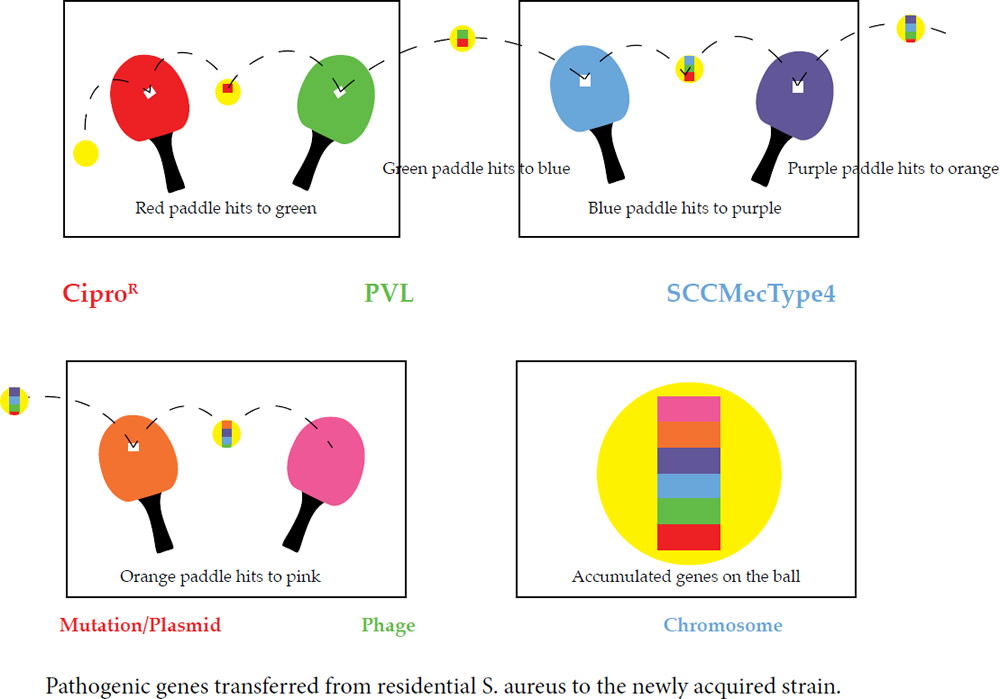
Figure 4. Ping-Pong Phenomenon: Ping-Pong MRSA “Evolution” refers to table tennis (ping-pong) as an illustration of genetic change in MRSA strains. If the ball hits a paddle with a sticky red strip, then hits another with a blue strip, and finally, a green strip, the end result would be a red, blue, and green strip all attached to the ball. In similar fashion, if a S. aureus coccus enters one person carrying unique DNA, then a second, and third person, the final person in a family may carry all 3 DNA strips, and thus, different MRSA isolates. This research adds to the knowledge base of how USA300 MRSA spreads throughout the country, and hints at how it emerges inside households and other shared spaces (gyms, etc). In like manner, a similar pattern may be happening in college close-knit dorms and communities, like those at Liberty University.
In the prestigious mBio journal, Alam et al. (2015) reported that they evaluated the samples to understand transmission dynamics, genetic relatedness, and microevolution of USA300 MRSA within households. For the study, researchers used genome sequencing on USA300 MRSA samples. These samples were collected during a previous study from 21 households in Chicago and Los Angeles where a family member had presented to the emergency room with a skin infection that was caused by USA300 MRSA. They created an evolutionary tree (fig. 5) to show the relationships among the bacterial strains. From a creation perspective, this “tree” shows variation and adaptation of S. aureus over the last decade.
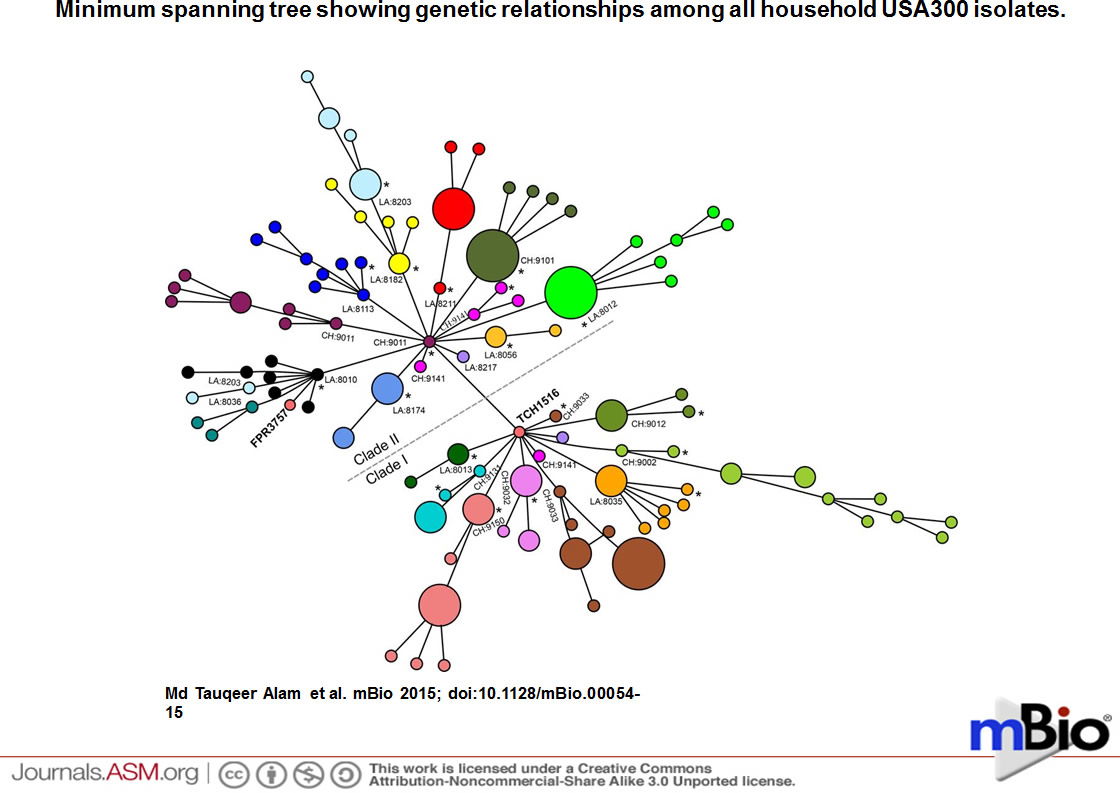
Figure 5. Evolutionary Tree for CA-MRSA. Minimum spanning tree showing genetic relationships among all household USA300 isolates. Each circle represents an individual genotype based on a 1,335,849-bp core gene alignment, and each color represents a different household. The size of the circle is proportional to the number of isolates with the genotype indicated. The household numbers are prefixed with CH (for Chicago) or LA (for Los Angeles). The index infection isolate in the household is indicated by an asterisk. The clades of USA300 strains with and without the grlA 80Y and gyrA 84L mutations are labeled clades I and II, respectively. As shown, the isolates from Los Angeles household 8203 split into two clusters but still remained in larger clade II. The isolates from Chicago household 9141 separated into two different clades with the presence or absence of grlA and gyrA mutations.
These Chicago researchers found that isolates within households clustered into closely related groups, suggesting a single common USA300 ancestral strain was introduced to and transmitted within each household. Researchers also determined from a technique using evolutionary reconstruction that USA300 MRSA persisted within households from 2 to 8 years before their samples were collected, and that in the course of a year, USA300 strains had a 1 in a million chance of having a random genetic change as a baseline, estimating the speed of change in these strains. Since bacteria reproduction rates are so high (generally less than 1 hour), this is not at all a major improbability. But researchers are seeing even more than would be expected due to random mutation; therefore, it is highly likely that positive selection is occurring. Researchers also found evidence that USA300 clones, when persisting in households, continued to acquire extraneous DNA.
This national study (Alam et al., 2015) demonstrates that USA300 MRSA strains within households were more similar to each other than those from different households. Although MRSA is rarely introduced into households, once there it can persist for years, “ping-ponging” (fig. 4) around from person to person. Their findings strongly suggest that unique USA300 MRSA isolates are transmitted within households that contain an individual with nasal carriage or skin infection (fig. 5). This research adds to the knowledge base of how USA300 MRSA spreads throughout the country, and hints at how it emerges inside households and other shared spaces (gyms, etc). In like manner, a similar pattern may be happening in college close-knit dorms, like those at Liberty University.
Genetic Change
The study by Alam et al. (2015) is important to healthcare and community alike. It is both a good study and a warning, wherein creation scientists would differ only in the use of some of the language of evolution. It is important for Christians because many believers are on the front lines of healthcare as physicians, nurses, physician assistants, and others in the health professions. The new CA-MRSA strains represent a danger due to their new dominance in the community, especially households and shared spaces of athletic teams. Staphylococcus aureus carried in high numbers contain a virulence factor that destroys leukocytes. The PVL Toxin gene facilitates destruction of neutrophils, macrophages, and in turn soft tissue and skin. This gene comes from a bacteriophage and now adds a virulence factor to the “Super” S. aureus.
The change is real and indicates the emergence of new MRSA variants, which some may describe as microevolution. The world of change in bacteria needs to be understood by both health care professionals and the creation biologist alike. However, this change is not upward, onward Darwinian evolution, but rather, an adaptive change as the species adjusts to its environment. This reshaping could be due to mutation, but the rapid diversification of MRSA among households (through the ping-pong effect) indicates that horizontal transfer through plasmid, or further yet, phage, is occurring. Again, it must be understood though, while this change makes new strains of MRSA more virulent and aggressive, this is not a case of upward-onward evolution. In order to survive against antibiotics, strains of MRSA that resist antibiotics have been “selected” at the cost of their own fitness. As MRSA picks up more genes to survive against antibiotics, it sacrifices some of its fitness to survive in its environment (more “foreign genes” acquired results in slower growth). The “new genes” are a temporary beneficial change for the bacteria, an adaptation in order to survive in a hostile environment.
Creation, the Fall, Super Staph, and MRSA
Where do the CA-MRSA microbes fit into God’s “very good” creation? Most creation biologists believe that God created (Genesis 1 and 2) all bacteria as very good forms of life (Gillen, 2009; 2015). The Creator most likely wove2 together man’s skin with a Staphylococcus kind. Perhaps, the original Staphylococcus kind diversified into several varieties according to microhabitat: some to live on the dry skin (primarily Staphylococcus epidermis) and some to live on moist skin, like Staphylococcus aureus, which frequently is carried harmlessly in the nose and occasionally colonizes the skin without harm (Gillen, Daycock, and Serafin, 2014).
Since the Fall, many bacteriophages and other genetic elements (plasmids) have invaded the original “very good” bacteria that are actually beneficial to us. Those toxins that are useful in the environment, having been displaced to the “wrong” location (that is the human body), have become dangerous. “Super” S. aureus evades the body defenses by secreting various enzymes to gain further expansion into the human body. For CA-MRSA, their toxins include leukocidins. The most dominant strains secrete a Panton Valentine leukocidin (PVL). PVL is associated with the majority of CA-MRSA strains in the USA and in particular MRSA USA300 strains. In addition, the added DNA codes for toxins and injurious chemicals that facilitate its spread across the skin, mucous membranes, and other body surfaces. The consequences to the staph invasion can then lead to harmful effects as discussed already (Tortora, Funke, and Case, 2015).
Community-associated MRSA infections are transmitted within a community that are not healthcare-related. But they can enter hospitals and are doing so. In the Chicago (2015) research study, they mostly looked at households. But the same seems to be occurring in athletic facilities and close-knit dorms. Any time there is skin contact from a carrier, or a fomite from a carrier, it can transmit. Extensive contact with lotions, soaps, cosmetics, towels, razors, hairbrushes, nail files, or athletic equipment increases risk of contraction. Those athletes in close physical contact (contact sports) have a higher risk. Those that have open cuts, wounds, etc. are even more susceptible. Those that visit clinics or hospitals have an even at higher risk both to themselves and to the community. At Liberty University, a number of student-athletes are in clinical majors such as nursing, health promotions, and biomedical majors. This may be one of the reasons for high MRSA carriage among students in our microbiology classes.
Evolution in Action?
So, is CA-MRSA really new and evolving? The specific strain, USA300 S. aureus, may be really new (from about 1997); however, pathogenic strains that are like it are probably not new. S. aureus has probably undergone significant change since its creation at the time of Genesis 1. God made all life with the ability to adapt to changing conditions; therefore, variation through time is the norm in microbes and all other creatures. In order to “survive,” S. aureus have mutated, changed, added genes, and adapted to their host.
Already-existing pathogenic genes, not novel genes, are transferred to residential skin or nasal S. aureus to produce a new strain. The mechanisms are not innovative and are limited in nature: these genes are new to S. aureus only. CA-MRSA is frequently more aggressive, virulent, and dangerous than the historical staph infection (methicillin sensitive S. aureus). The change in MRSA is occurring, and as it could possibly become more dangerous, more research is needed on the mechanisms of transfer and change in the new strains of MRSA to confront this threat. Is the ping-pong phenomenon and new variants of S. aureus an example of evolution in action? No, if one is referring to an upward, onward evolution.
The changes seen S. aureus are primarily due to a series of horizontal transfers and adaptations. There is variation to meet the demand of the new environment. One can readily observe changes like these in other pathogens and parasites. The ping-pong phenomena might be described as microevolution, variation, or horizontal evolution, but none of the changes lead to upward, onward Darwinian macroevolution. Regardless of the language, it is medically important for those combating infectious and parasitic diseases.
Definitions
- Ciprofloxacin (Cipro)
- Ciprofloxacin (Cipro) is an antibiotic that can treat a number of bacterial infections. It is a second-generation fluoroquinolone.
- MRSA Carriage (Colonization)
- MRSA Carriage (Colonization) is different than MRSA invasive disease (an infection).
- Phage
- A virus that parasitizes a bacterium by infecting it and reproducing inside it. (New Oxford American Dictionary)
- Plasmid
- A genetic structure in a cell that can replicate independently of the chromosomes, typically a small circular DNA strand in the cytoplasm. (New Oxford American Dictionary)
- Fomite
- Objects or materials that are likely to carry infection, such as clothes, utensils, and furniture.
- Leukocidin
- A toxin that destroys leukocytes.
References
Alam, M.T., T.D. Read, R.A. Petit III, S. Boyle-Vavra, L.G. Miller, S.J. Eells, R.S. Daum, M.Z. David. 2015. “Transmission and Microevolution of USA300 MRSA in U.S. Households: Evidence from Whole-Genome Sequencing.” mBio 6 (2): e00054–15. doi:10.1128/mBio.00054-15.
American Society for Microbiology. 2015. “MRSA Can Linger in Homes, Spreading among Its Inhabitants.” ScienceDaily. http://www.sciencedaily.com/releases/2015/03/150310074434.htm.
Fox, J., ed. 2015. The Threat of MRSA. American Academy of Microbiology. Washington, DC.
Gillen, A. L. 2015. The Genesis of Germs: Disease and the Coming Plagues in a Fallen World. Green Forest, Arkansas: Master Books.
Gillen, A. L. 2014. “The Wonderfully Made Design of the Skin and Its Microbiome.” Answers in Depth 9. https://answersingenesis.org/human-body/wonderfully-made-design-skin-and-its-microbiome/.
Gillen, A., W. Daycock, and A. Serafin. 2014. “High MRSA Carriage Rate among Nursing Microbiology Students.” Advances in Microbiology, 4: 871–877. http://dx.doi.org/10.4236/aim.2014.413096.
Tortora, G.J., B. R. Funke, and C. L. Case. 2015. Microbiology: An Introduction. 12th ed. Pearson Benjamin/Cummings Pub. Co. San Francisco, CA.

Footnotes
- Staphylococcal cassette chromosome mec, which includes the mecA gene coding for resistance to methicillin.
- Wove together—this implies a mutualistic relationship between two distinct organisms, not a mosaic of one.
{kind=link}
Support the creation/gospel message by donating or getting involved!

Answers in Genesis is an apologetics ministry, dedicated to helping Christians defend their faith and proclaim the good news of Jesus Christ.
- Customer Service 800.778.3390
- © 2024 Answers in Genesis